Galectin-3: The Architect of Cardiac Issues
In cardiovascular medicine, Galectin-3 (Gal-3) is often referred to as a "culprit" biomarker. Unlike many markers that simply indicate a problem (bystanders), Gal-3 actively drives the progression of heart failure and tissue scarring.
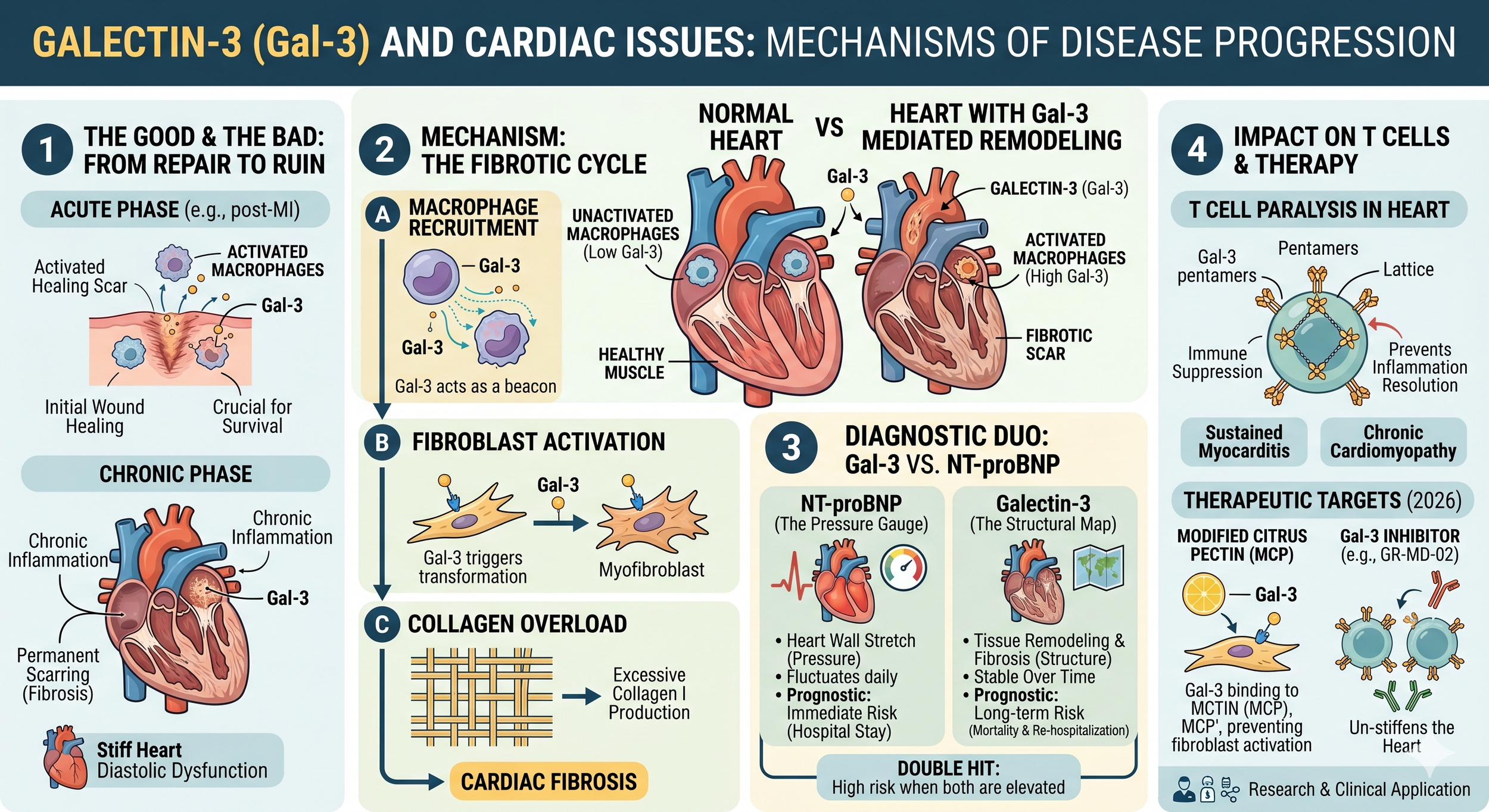
1. From Repair to Ruin: The Two Faces of Gal-3
In a healthy heart, Gal-3 levels are virtually undetectable. However, when the heart is injured (e.g., during a heart attack), Gal-3 is rapidly released by activated macrophages to begin the repair process.
The Good (Acute Phase): Gal-3 helps in initial wound healing after a Myocardial Infarction (MI). In Gal-3 "knockout" mice, the heart fails to form a proper scar, often leading to cardiac rupture.
The Bad (Chronic Phase): If Gal-3 levels stay high, it triggers chronic inflammation and permanent scarring (fibrosis). This stiffens the heart muscle, making it harder to pump blood, eventually leading to heart failure.
2. Mechanism: How Gal-3 Scarring Works
Gal-3 acts as a signaling bridge between immune cells and the structural cells of the heart:
Macrophage Recruitment: Gal-3 acts as a "chemical beacon" (chemoattractant), pulling more inflammatory monocytes into the heart tissue.
Fibroblast Activation: It binds to receptors on cardiac fibroblasts, turning them into highly active "myofibroblasts."
Collagen Overload: These myofibroblasts pump out excessive amounts of Type I collagen. While some collagen is needed for a scar, too much of it creates a "stiff heart" (diastolic dysfunction).
3. Gal-3 vs. NT-proBNP: What’s the Difference?
In clinical practice, doctors often view Galectin-3 and NT-proBNP as two different lenses through which to view the heart. While NT-proBNP acts like a "pressure gauge," measuring the immediate stretch and strain on the heart walls, it can fluctuate rapidly based on daily fluid intake or medication. In contrast, Galectin-3 acts more like a "structural map." It reflects the underlying biological process of tissue remodeling and permanent scarring.
Because Gal-3 levels are relatively stable over time, they provide a more consistent look at long-term damage rather than immediate distress. When both markers are elevated, it signals a high-risk "double hit": the heart is both under high physical pressure and actively turning its healthy muscle into non-functional scar tissue. This combination is a strong predictor of long-term mortality and frequent re-hospitalization.4. Impact on T Cells in the Heart
Just like in cancer, Gal-3 can "paralyze" the immune response in the heart, but with a different outcome:
Suppressed Resolution: By creating a "lattice" on T cells, Gal-3 can prevent the immune system from transitioning from the "inflammatory" phase to the "resolution" phase.
Sustained Myocarditis: In cases of heart inflammation (myocarditis), Gal-3 keeps T cells in a state of dysfunction, preventing the heart from fully clearing the inflammation and leading to chronic dilated cardiomyopathy.
5. Therapeutic Targets in 2026
Recent clinical trials are focusing on blocking Gal-3 to stop heart failure before it becomes irreversible:
Modified Citrus Pectin (MCP): A natural Gal-3 inhibitor that binds to the protein's "sugar-loving" site, preventing it from activating fibroblasts.
GR-MD-02: Originally for liver fibrosis, this drug is being explored to see if it can "un-stiffen" the heart by breaking the Gal-3 signaling cycle.
Key Takeaway: If Gal-3 is high in a cardiac patient, it usually means the heart's architecture is being actively remodeled into scar tissue. Lowering Gal-3 isn't just about the "score"—it's about stopping the heart from turning into a stiff, non-functional pump.
Scientific Foundations: The Evidence for Galectin-3 and Cardiac Issues
-
![]()
Journal: Circulation
Galectin-3 marks activated macrophages in failure-prone hypertrophied hearts and contributes to cardiac dysfunction (2004)
-
![]()
Journal: European Journal of Heart Failure
Galectin-3: A novel mediator of heart failure development and progression (2009)
-
![]()
Journal: Circulation: Heart Failure
Genetic and pharmacological inhibition of galectin-3 prevents cardiac remodeling by interfering with myocardial fibrogenesis (2013)
-
![]()
Journal: Circulation: Heart Failure
Prognostic value of changes in galectin-3 levels over time in patients with heart failure (2013)
-
![]()
Journal: Curr Heart Fail Rep
Galectin-3 in Cardiac Remodeling and Heart Failure (2010)