The Brain's Double Agent: The Dual Role of Galectin-3 in Stroke
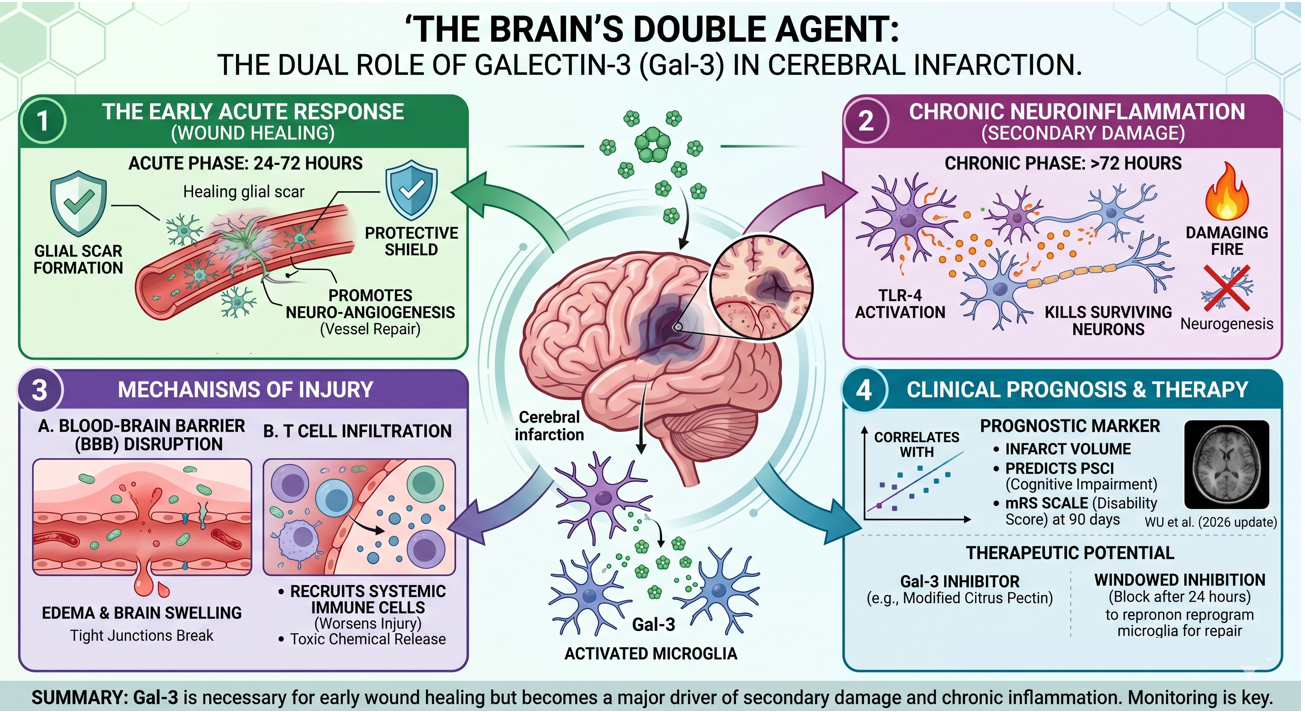
In the context of neurology, Galectin-3 (Gal-3) has emerged as a critical biomarker and biological driver for Cerebral Infarction (Ischemic Stroke). Much like its role in the heart, Gal-3 in the brain acts as a double-edged sword: it is essential for early wound healing but becomes a major cause of secondary damage and long-term disability when chronically elevated.
1. The Brain's "Damage Signal"
Following a cerebral infarction, the brain’s resident immune cells (microglia) become activated. These cells are the primary source of Gal-3 in the central nervous system.
Acute Response: Within 24–72 hours of a stroke, Gal-3 levels spike. It helps stabilize the damaged area by promoting the formation of a "glial scar," which prevents the injury from spreading to healthy brain tissue.
Chronic Neuroinflammation: If Gal-3 remains high, it shifts microglia into a "pro-inflammatory" state. This creates a cycle of chronic inflammation that kills surviving neurons and prevents the brain from repairing its neural connections (neurogenesis).
2. Mechanisms of Injury in Stroke
Gal-3 contributes to the severity of a cerebral infarction through several specific pathways:
Blood-Brain Barrier (BBB) Disruption: High levels of Gal-3 promote the breakdown of the tight junctions between cells in the brain's blood vessels. This leads to cerebral edema (brain swelling), which is a leading cause of death in the days following a major stroke.
T Cell Infiltration: Just as Gal-3 interacts with T cells in tumors, in the brain, it helps "recruit" systemic immune cells into the stroke site. While this sounds helpful, these cells often release toxic chemicals that worsen the "infarct volume" (the size of the dead tissue area).
Pro-thrombotic State: Some research suggests Gal-3 may interact with platelets, potentially increasing the "stickiness" of the blood and making secondary strokes more likely.
3. Clinical Significance: Predicting the Outcome
Gal-3 is now being used as a "prognostic" marker to tell doctors how well a patient might recover from a stroke.
Infarct Size Correlation: Clinical studies show a direct correlation between serum Gal-3 levels and the volume of the brain lesion seen on an MRI. Higher Gal-3 = larger infarction.
Predicting Post-Stroke Outcome: Patients with high Gal-3 levels at the time of admission are statistically more likely to suffer from "Post-Stroke Cognitive Impairment" (PSCI) and have lower scores on the modified Rankin Scale (a measure of disability) 90 days after the event.
Hemorrhagic Transformation: High Gal-3 is a risk factor for "hemorrhagic transformation"—a dangerous complication where an ischemic stroke begins to bleed.
4. Gal-3 vs. Traditional Stroke Markers
While proteins like NSE (Neuron-Specific Enolase) tell us how many neurons have already died, Gal-3 tells us about the inflammatory environment of the brain.
NSE: Measures immediate cell death.
Gal-3: Measures the intensity of the body's inflammatory reaction, which determines how much more damage will happen in the week following the stroke.
5. Therapeutic Potential: "The Neuro-Protective Target"
Research in 2025 and 2026 is investigating whether blocking Gal-3 immediately after a stroke can save brain tissue.
Modified Citrus Pectin (MCP): Animal models have shown that administering Gal-3 inhibitors shortly after a stroke can reduce brain swelling and limit the final size of the infarct.
Microglial Modulation: By blocking Gal-3, scientists hope to "re-program" microglia back into a "repair" mode, encouraging the growth of new synapses (plasticity).
Scientific Foundations: The Evidence for Galectin-3 and Ischemic Stroke
-
![]()
Journal: Aging
The serum galectin-3 levels are associated with the severity and prognosis of ischemic stroke (2021)
-
![]()
Journal: Mediators of Inflammation
Galectin-3: A Novel Marker for the Prediction of Stroke Incidence and Clinical Prognosis (2022)
-
![]()
Journal: Neurointerventional Surgery
Dynamic Changes and Clinical Significance of Plasma Galectin-3 in Patients with AIS Undergoing Endovascular Therapy (2024)
-
![]()
Journal: Cerebral Blood Flow & Metabolism
Galectin-3 protects against ischemic stroke by promoting neuro-angiogenesis via apoptosis inhibition and Akt/Caspase regulation (2021)